

Introduction: Acquired thrombotic thrombocytopenic purpura (TTP) is a life-threatening disease characterized by thrombotic microangiopathy leading to end-organ damage. The standard of care (SOC) treatment is therapeutic plasma exchange (TPE) alongside immunomodulation with steroids, with increasing use of rituximab +/- other immunomodulatory agents. The addition of caplacizumab, a nanobody targeting von Willebrand factor, was shown to accelerate platelet count recovery, reduce TPE treatments and hospital length of stay, decrease exacerbations and increase relapses in TTP patients treated in the TITAN and HERCULES trials. Given the efficacy of caplacizumab in the TITAN and HERCULES trials, we conducted a cost effectiveness analysis (CEA) of caplacizumab in acquired TTP, representing the first-ever CEA in TTP.
Methods: We built decision tree models to evaluate the cost effectiveness of SOC plus caplacizumab versus SOC in acquired TTP based on the results of each of the phase II TITAN trial at 12-month follow-up and the phase III HERCULES trial at 1-month follow-up. Costs were assessed from the health system perspective. For each trial, the SOC cost was calculated as the sum of TPE sessions, hospital length-of-stay (LOS), intensive care unit (ICU) stay, and rituximab use, while the cost of the SOC plus caplacizumab arm included the SOC cost plus the list price of caplacizumab (USD $270,000 per TTP episode). Effectiveness was calculated in quality-adjusted life years (QALY). Cost effectiveness of each treatment arm was calculated as the ratio of cost divided by QALYs. The incremental cost effectiveness ratio (ICER) of adding caplacizumab to SOC was calculated as the difference between the costs of the two treatment arms divided by the difference in QALYs; the ICER was then compared against the 2019 US willingness-to-pay (WTP) threshold of $195,300 USD as a measure of overall cost effectiveness. To avoid potential confounding factors that might inadvertently bias our analysis against the addition of caplacizumab, all values used in our models were selected to maximize cost in the SOC arm and minimize cost in the SOC plus caplacizumab arm in the two clinical trials. We also created a Markov model comparing cost effectiveness of SOC plus caplacizumab versus SOC in acquired TTP with a 5-year time horizon. We performed one-way sensitivity analyses for all models varying parameters including LOS, ICU stay, number of TPE sessions, rituximab use, utilities of the well and diseases states, and caplacizumab cost.
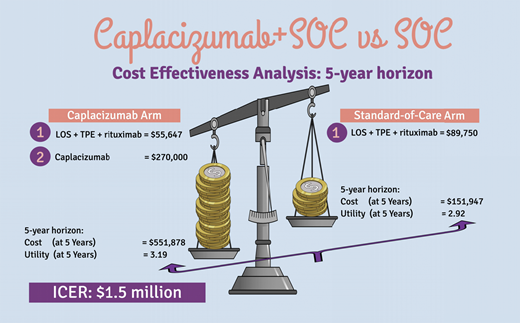
Results: In the decision tree models, caplacizumab use yielded a higher cost of treatment compared to SOC alone in both trials (TITAN: $325,647 for caplacizumab plus SOC, versus $89,750 for SOC; HERCULES: $323,547 for caplacizumab plus SOC, versus $83,634 for SOC). An improvement in QALYs with the addition of caplacizumab was noted as compared to SOC in both trials (0.07 in TITAN and 0.26 in HERCULES). The ICER for adding caplacizumab to SOC versus SOC alone was $3.7 million in the TITAN trial and $0.9 million in the HERCULES trial, well above the US WTP threshold. The 5-year horizon Markov model yielded higher cost of caplacizumab treatment compared to SOC alone ($551,878 versus $151,947) and an improvement in QALYs (3.19 versus 2.92). The ICER for adding caplacizumab to SOC was $1.5 million (95% confidence interval $1.25-$1.72 million) with SOC favored in 100% of 10,000 Monte Carlo simulations in a probabilistic sensitivity analysis. Among all parameters, decreasing the cost of caplacizumab had the greatest impact on decreasing the ICERs in all models. The price of caplacizumab treatment for one TTP episode to meet the 2019 US WTP would have to be $46,424 and $80,848 in the TITAN and HERCULES decision tree models, respectively, and $65,106 in a Markov model with a 5-year horizon.
Conclusion: The addition of caplacizumab to SOC treatment is not cost effective at its current drug pricing. As our models are designed to maximize the cost effectiveness of caplacizumab, it is very likely that the actual costs incurred by this medication will be much higher than what we report here. Compared to CEA studies of other orphan drugs that, unlike caplacizumab, alter long-term disease course, the costs incurred by caplacizumab treatment in acquired TTP are at the higher end of the spectrum. Additional studies utilizing longer-term follow-up data are warranted to assess the full impact of caplacizumab on the cost of treating TTP.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal